






Will High Testosterone Cause Your Psa To Go Up
What are male sex hormones?
Hormones are substances that are made by glands in the body. Hormones circulate in the bloodstream and control the actions of certain cells or organs.
Androgens (male sex hormones) are a class of hormones that control the development and maintenance of male characteristics. The most abundant androgens in men are testosterone and dihydrotestosterone (DHT).
Androgens are required for normal growth and function of the prostate, a gland in the male reproductive system that helps make semen. Androgens are also necessary for prostate cancers to grow. Androgens promote the growth of both normal and cancerous prostate cells by binding to and activating the androgen receptor, a protein that is expressed in prostate cells (1). Once activated, the androgen receptor stimulates the expression of specific genes that cause prostate cells to grow (2).
Almost all testosterone is produced in the testicles; a small amount is produced by the adrenal glands. Although prostate cells do not normally make testosterone, some prostate cancer cells acquire the ability to do so (3).
How does hormone therapy work against prostate cancer?
Early in their development, prostate cancers need androgens to grow. Hormone therapies, which are treatments that decrease androgen levels or block androgen action, can inhibit the growth of such prostate cancers, which are therefore called castration sensitive, androgen dependent, or androgen sensitive.
Most prostate cancers eventually stop responding to hormone therapy and become castration (or castrate) resistant. That is, they continue to grow even when androgen levels in the body are extremely low or undetectable. In the past, these tumors were also called hormone resistant, androgen independent, or hormone refractory; however, these terms are rarely used now because the tumors are not truly independent of androgens for their growth. In fact, some newer hormone therapies have become available that can be used to treat tumors that have become castration resistant.
What types of hormone therapy are used for prostate cancer?
Hormone therapy for prostate cancer can block the production or use of androgens (4). Currently available treatments can do so in several ways:
- reducing androgen production by the testicles
- blocking the action of androgens throughout the body
- block androgen production (synthesis) throughout the body
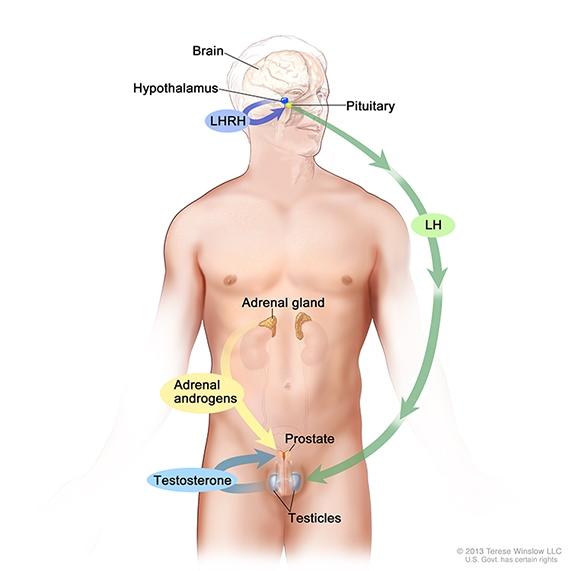
Androgen production in men. Drawing shows that testosterone production is regulated by luteinizing hormone (LH) and luteinizing hormone-releasing hormone (LHRH). The hypothalamus releases LHRH, which stimulates the release of LH from the pituitary gland. LH acts on specific cells in the testes to produce the majority of testosterone in the body. Most of the remaining androgens are produced by the adrenal glands. Androgens are taken up by prostate cells, where they either bind to the androgen receptor directly or are converted to dihydrotestosterone (DHT), which has a greater binding affinity for the androgen receptor than testosterone.
Treatments that reduce androgen production by the testicles are the most commonly used hormone therapies for prostate cancer and the first type of hormone therapy that most men with prostate cancer receive. This form of hormone therapy (also called androgen deprivation therapy, or ADT) includes:
- Orchiectomy, a surgical procedure to remove one or both testicles. Removal of the testicles, called surgical castration, can reduce the level of testosterone in the blood by 90% to 95% (5). A type of orchiectomy called subcapsular orchiectomy removes only the tissue in the testicles that produces androgens, rather than the entire testicle. Orchiectomy is permanent and irreversible.
- Drugs called luteinizing hormone-releasing hormone (LHRH) agonists, which prevent the pituitary gland from secreting a hormone called luteinizing hormone. LHRH agonists, which are sometimes called LHRH analogs, are synthetic proteins that are structurally similar to LHRH and bind to the LHRH receptor in the pituitary gland. (LHRH is also known as gonadotropin-releasing hormone or GnRH, so LHRH agonists are also called GnRH agonists or GnRH analogs.)
Normally, when androgen levels in the body are low, the hypothalamus releases LHRH. This stimulates the pituitary gland to produce luteinizing hormone, which in turn stimulates the testicles to produce androgens. LHRH agonists, like the body's own LHRH, initially stimulate the production of luteinizing hormone. However, the continued presence of high levels of LHRH agonists actually causes the pituitary gland to stop producing luteinizing hormone. As a result, the testicles are not stimulated to produce androgens.
Treatment with an LHRH agonist is called medical castration or chemical castration. But, unlike surgical castration (orchiectomy), the effects of these drugs on androgen production are reversible. Once treatment is stopped, androgen production usually resumes.
LHRH agonists are given by injection or are implanted under the skin. Four LHRH agonists are approved to treat prostate cancer in the United States: leuprolide (Lupron), goserelin (Zoladex), triptorelin (Trelstar), and histrelin (Vantas).
When patients receive an LHRH agonist for the first time, they may experience a phenomenon called "testosterone flare." This temporary increase in testosterone level occurs because LHRH agonists briefly cause the pituitary gland to secrete extra luteinizing hormone before blocking its release. The flare may worsen clinical symptoms (such as bone pain, ureter or bladder outlet obstruction, and spinal cord compression). The increase in testosterone is usually countered by giving another type of hormone therapy, called antiandrogen therapy, along with the LHRH agonist for the first few weeks of treatment.
- Drugs called LHRH antagonists, which are another form of medical castration. LHRH antagonists (also called GnRH antagonists) prevent LHRH from binding to its receptors in the pituitary gland. This prevents the secretion of luteinizing hormone, which stops the testicles from producing androgens. Unlike LHRH agonists, LHRH antagonists do not cause a testosterone flare.
Two LHRH antagonists are approved to treat advanced prostate cancer in the United States: degarelix (Firmagon) is given by injection, and relugolix (Orgovyx) is a pill that is taken by mouth.
- Estrogens (hormones that promote female sex characteristics). Although estrogens are also able to inhibit androgen production by the testicles, they are seldom used today in the treatment of prostate cancer because of their side effects.
Treatments that block the action of androgens in the body (also called antiandrogen therapies) are typically used when ADT stops working. Such treatments include:
- Androgenreceptor blockers (also called androgen receptor antagonists), which are drugs that compete with androgens for binding to the androgen receptor. By competing for binding to the androgen receptor, these treatments reduce the ability of androgens to promote prostate cancer cell growth.
Because androgen receptor blockers do not prevent androgen from being produced, they are not commonly used on their own to treat prostate cancer. Instead, they are usually used in combination with ADT (either orchiectomy or an LHRH agonist). Use of an androgen receptor blocker in combination with orchiectomy or an LHRH agonist is called combined androgen blockade, complete androgen blockade, or total androgen blockade.
Androgen receptor blockers that are approved in the United States to treat prostate cancer include the first-generation drugs flutamide, bicalutamide (Casodex), and nilutamide (Nilandron), and the second-generation drugs enzalutamide (Xtandi), apalutamide (Erleada), and darolutamide (Nubeqa), which bind and block the androgen receptor more strongly and specifically than the first-generation drugs (6). Of these, only darolutamide does not cross the blood-brain barrier in humans, which may result in fewer central nervous system–related side effects. They are given as pills to be swallowed.
Treatments that block the production of androgens throughout the body include:
- Androgen synthesis inhibitors, which are drugs that prevent the production of androgens by all tissues that produce them. Neither medical nor surgical castration prevents the adrenal glands and prostate cancer cells from producing androgens. Even though these cells produce only small amounts of androgens, they can be enough to support the growth of some prostate cancers.
Androgen synthesis inhibitors lower testosterone levels in a man's body to a greater extent than any other known treatment. They do so by inhibiting an enzyme called CYP17. This enzyme, which is found in testicular, adrenal, and prostate tumor tissues, is necessary for the body to produce testosterone from cholesterol.
Three androgen synthesis inhibitors are approved in the United States: abiraterone (Yonsa, Zytiga), ketoconazole, and aminoglutethimide. All are given as pills to be swallowed.
Abiraterone is approved in combination with prednisone to treat metastatic prostate cancer, both castration-sensitive and castration-resistant. Before the approval of abiraterone and enzalutamide, two drugs that are approved for indications other than prostate cancer (ketoconazole and aminoglutethimide) were sometimes used off-label as second-line treatments for castration-resistant prostate cancer.
How is hormone therapy used to treat hormone-sensitive prostate cancer?
Hormone therapy may be used in several ways to treat hormone-sensitive prostate cancer, including:
Early-stage prostate cancer with an intermediate or high risk of recurrence. Men with early-stage prostate cancer that has an intermediate or high risk of recurrence often receive hormone therapy before, during, and/or after radiation therapy, or after prostatectomy (surgery to remove the prostate gland) (7). Factors that are used to determine the risk of prostate cancer recurrence include the grade of the tumor (as measured by the Gleason score), the extent to which the tumor has spread into surrounding tissue, and whether tumor cells are found in nearby lymph nodes during surgery.
The use of hormone therapy (alone or in combination with chemotherapy) before prostatectomy has not been shown to be of benefit and is not a standard treatment. More intensive androgen blockade prior to prostatectomy is being studied in clinical trials.
Relapsed/recurrent prostate cancer. Hormone therapy used alone is the standard treatment for men who have a prostate cancer recurrence as documented by CT, MRI, or bone scan after treatment with radiation therapy or prostatectomy.
Hormone therapy is sometimes recommended for men who have a "biochemical" recurrence—a rise in prostate-specific antigen (PSA) level following primary local treatment with surgery or radiation—especially if the PSA level doubles in fewer than 3 months.
Advanced or metastatic prostate cancer. ADT used alone was for many years the standard treatment for men who are found to have metastatic disease (i.e., disease that has spread to other parts of the body) when their prostate cancer is first diagnosed (8). More recently, clinical trials have shown that such men survive longer when treated with ADT plus another type of hormone therapy (abiraterone/prednisone, enzalutamide, or apalutamide) than when treated with ADT alone (9–17).
In addition, an NCI-sponsored trial showed that men with hormone-sensitive metastatic prostate cancer lived longer when treated with the chemotherapy drug docetaxel (Taxotere) at the start of ADT than men treated with ADT alone (18). Men with the most extensive metastatic disease appeared to benefit the most from the early addition of docetaxel.
Although hormone therapy can delay progression of disease and may be able to prolong survival, it can also have substantial side effects. Men should discuss the risks and potential benefits of hormone therapy with their doctor in light of their own medical concerns.
Palliation of symptoms. Hormone therapy is sometimes used alone for palliation or prevention of local symptoms in men with localized prostate cancer who are not candidates for surgery or radiation therapy (19). Such men include those with a limited life expectancy, those with locally advanced tumors, and/or those with other serious health conditions.
How will I know that my hormone therapy is working?
Doctors cannot predict how long hormone therapy will be effective in suppressing the growth of any individual man's prostate cancer. Therefore, men who take hormone therapy for more than a few months are regularly tested to determine the level of PSA in their blood. An increase in PSA level may indicate that a man's cancer has started growing again. A PSA level that continues to increase while hormone therapy is successfully keeping androgen levels extremely low is an indicator that a man's prostate cancer has become resistant to the hormone therapy that is currently being used.
How is castration-resistant prostate cancer treated?
Treatments for castration-resistant prostate cancer include:
- Complete androgen blockade—that is, androgen receptor blockers (flutamide, bicalutamide, nilutamide, apalutamide, darolutamide, or enzalutamide).
- Androgen synthesis inhibition with abiraterone.
- Immunotherapy using a cell-based vaccine called sipuleucel-T (Provenge). This vaccine uses a man's own immune cells to fight metastatic prostate cancer that has few or no symptoms.
- Chemotherapy, most commonly with the drug docetaxel. Another drug, cabazitaxel (Jevtana), is approved for the treatment of metastatic castration-resistant prostate cancer that was previously treated with docetaxel.
- Radium-223 dichloride (Xofigo), a radiopharmaceutical that collects in areas of bone that are undergoing increased turnover (bone resorption coupled with bone formation), such as where bone metastases are forming, and gives off radiation that kills cancer cells.
- Drugs that inhibit an enzyme called PARP, which helps repair DNA when it becomes damaged. Two PARP inhibitors, rucaparib camsylate (Rubraca) and olaparib (Lynparza), are used to treat castration-resistant prostate cancers that have certain mutations.
Men with castration-resistant prostate cancer who receive these treatments will continue to receive ADT (e.g., an LHRH agonist) to keep testosterone levels low, because an increase in testosterone could lead to tumor progression in some men (20).
Randomized clinical trials in men with metastatic castration-resistant prostate cancer have shown improved survival among men receiving abiraterone or enzalutamide in addition to ADT compared with those receiving ADT alone, whether or not they have previously received chemotherapy (11, 12, 15–17).
Similarly, in randomized clinical trials, men with nonmetastatic castration-resistant prostate cancer who received apalutamide, enzalutamide, or darolutamide in addition to ADT lived longer than those who received ADT alone (21–23).
What is intermittent ADT?
Researchers have investigated whether a technique called intermittent androgen deprivation can delay the development of hormone resistance. With intermittent androgen deprivation, hormone therapy is given in cycles with breaks between drug administrations, rather than continuously. An additional potential benefit of this approach is that the temporary break from the side effects of hormone therapy may improve a man's quality of life.
Randomized clinical trials have shown similar overall survival with continuous ADT or intermittent ADT among men with metastatic or recurrent prostate cancer, with a reduction in some side effects for intermittent ADT (24–26).
What are the side effects of hormone therapy for prostate cancer?
Because androgens affect many other organs besides the prostate, ADT can have a wide range of side effects (4, 27), including:
- loss of interest in sex (lowered libido)
- erectile dysfunction
- hot flashes
- loss of bone density
- bone fractures
- loss of muscle mass and physical strength
- changes in blood lipids
- insulin resistance
- weight gain
- mood swings
- fatigue
- growth of breast tissue (gynecomastia)
Antiandrogens can cause diarrhea, breast tenderness, nausea, hot flashes, loss of libido, and erectile dysfunction. The antiandrogen flutamide may damage the liver, and enzalutamide and apalutamide may cause fractures. Darolutamide may avoid some central nervous system–related side effects seen with enzalutamide and apalutamide, such as seizures and falls.
Androgen synthesis inhibitors can cause diarrhea, itching and rashes, fatigue, erectile dysfunction (with long-term use), and, potentially, liver damage.
Estrogens avoid the bone loss seen with other kinds of hormone therapy, but they increase the risk of cardiovascular side effects, including heart attacks and strokes. Because of these side effects, estrogens are rarely used today as hormone therapy for prostate cancer.
Although the addition of ADT to radiation therapy has been shown to increase survival for men with high-risk prostate cancer, it worsens some adverse effects of radiotherapy, particularly sexual side effects and vitality (28). Many of the side effects of ongoing hormone therapy also become stronger the longer a man takes hormone therapy (27).
What can be done to reduce the side effects of hormone therapy for prostate cancer?
Men who lose bone mass during long-term hormone therapy may be prescribed drugs to slow or reverse this loss. The drugs zoledronic acid (Zometa) and alendronate (Fosamax) (both of which belong to a class of drugs called bisphosphonates) can be used to increase bone mineral density in men who are undergoing hormone therapy (29, 30), as can a newer drug, denosumab (Prolia), which increases bone mass through a different mechanism (31). However, drugs to treat bone loss are associated with a rare but serious side effect called osteonecrosis of the jaw (20).
Exercise may help reduce some of the side effects of hormone therapy, including bone loss, muscle loss, weight gain, fatigue, and insulin resistance (20, 32). Several clinical trials are examining whether exercise can reverse or prevent side effects of hormone therapy for prostate cancer.
The sexual side effects of hormone therapy for prostate cancer can be some of the most difficult to deal with. Erectile dysfunction drugs such as sildenafil (Viagra) do not usually work for men undergoing hormone therapy because these drugs do not address the loss of libido (sexual desire) that is associated with a lack of androgens.
More information about the sexual side effects of cancer treatment can be found on theSexual Health Issues in Men with Cancer page.
Most of the sexual and emotional side effects caused by low levels of androgens will eventually go away if a man stops taking hormone therapy. However, particularly for older men and those who received ADT for a long time, testosterone levels may not fully recover and these side effects may not disappear completely. Some physical changes that have developed over time, such as bone loss, will remain after stopping hormone therapy.
Patients should be sure to tell their doctor about all medications and supplements they are taking, including over-the-counter herbal medicines. Some herbal medicines interact with drug metabolizing enzymes in the body, which can adversely affect hormone therapy (33).
Get Help Finding Clinical Trials of Hormone Therapy for Prostate Cancer
Call NCI's Cancer Information Service at 1-800-4-CANCER (1-800-422-6237) for information about clinical trials of hormone therapy for prostate cancer.
Will High Testosterone Cause Your Psa To Go Up
Source: https://www.cancer.gov/types/prostate/prostate-hormone-therapy-fact-sheet






Tidak ada komentar:
Posting Komentar